Preferred Sample Type
")
Suitable Specimen Types
- Faeces
Specimen Transport
Usual to laboratoryTurnaround Time
7 working daysSample Stability
Upon receipt store sample below -18̊C ready for extraction. Extracted samples are stored between 2-8̊C prior to analysisCalprotectin (faecal)
General Information
Calprotectin is a protein found in cells involved in inflammation. It is present in abundance in neutrophils. The concentration of calprotectin in faeces is increased in inflammatory bowel disease and has been shown to be a better marker of the disease activity (seen on tissue biopsy) than blood test markers of inflammation (e.g. white blood cell count, ESR and CRP). Its measurement is relatively cheap, non-invasive and it is stable in faeces at room temperature for several days.
The main diseases that cause an increased excretion of faecal calprotectin are Crohn's disease, ulcerative colitis and cancer. Levels of faecal calprotectin are not raised in patients with irritable bowel syndrome (IBS).
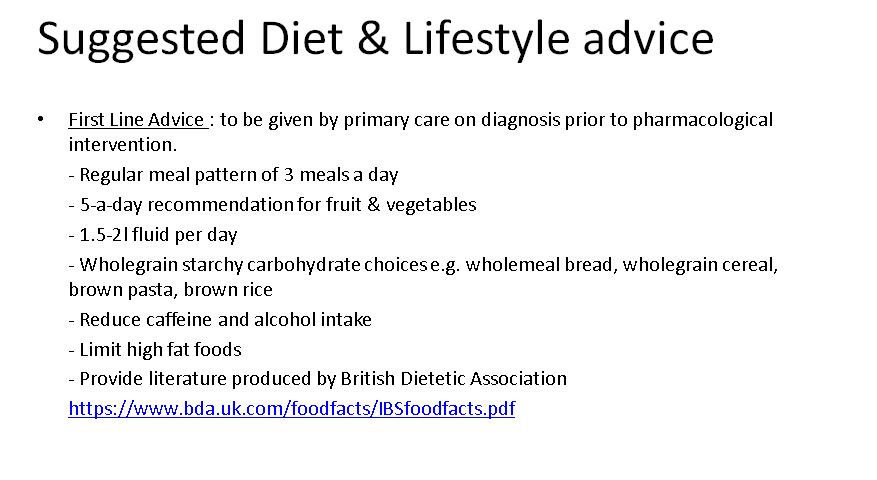
Patient Preparation
>Random faecal sample (any time of day, no dietary restrictions required) in a plain universal container and approximately 1 gram in weight.
Notes
Please note, from 17th October 2016, specimens will be processed at HEFT using the Buhlmann fCAL (TM) Turbo assay.
NB: Reference range and guidelines applicable to adult patients only, as agreed locally with gastroenterologists.
Reference Range
Reference ranges from 17/10/2016 (NB: reference range only applicable to adult patients):
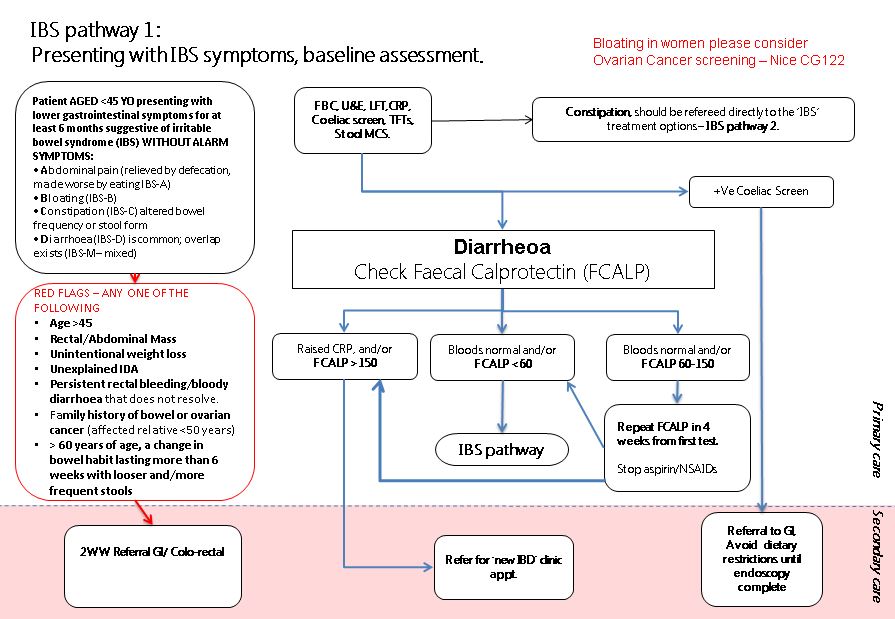
≤60ug/g: Not indicative of GI inflammation
>60ug/g but ≤ 150ug/g: Moderately elevated levels are associated with organic intestinal disease but should be interpreted in line with clinical assessment. Repeat FCALP in 4 weeks from first test and stop aspirin/NSAIDs. If this is the repeat test please refer for ‘new IBD’ clinic appointment.
>150ug/g: Elevated calprotectin suggestive of but not diagnostic of inflammatory bowel disease. Please refer for ‘new IBD’ clinic appointment.
Please see guidelines for adult patients below:
Source of Reference Range
Agreed with Consultant Gastroenterologists to be used in in conjunction with local IBS guidelinesSpecifications
- EQA Scheme?: Yes